IOL Calculation Formulas Explained: SRK/T, Haigis, Holladay, Hoffer Q, and Barrett Universal II
A practical guide to selecting the right IOL formula for each patient — when to use Barrett Universal II vs SRK/T, how axial length and keratometry affect formula choice, and what the evidence says about accuracy in short, normal, and long eyes
Why formula selection matters
Cataract surgery achieves a refractive outcome within ±0.5 D of the target in 70–85% of cases with modern formulas — but that range depends heavily on choosing the right formula for the eye's biometric profile. The difference between a good outcome and a disappointed patient often comes down to which formula you use for an axial length of 26.5 mm or a flat K reading of 40.5 D.
This guide is written for ophthalmologists who want to understand the practical differences between the five most-used formulas — not the mathematics, but the clinical decisions.
The five formulas and what drives them
SRK/T — The universal baseline
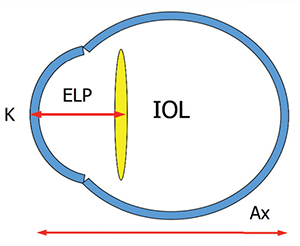
The Sanders-Retzlaff-Kraff/Theoretical formula, published in 1990, is a regression-empirical hybrid that uses axial length (AL) and mean keratometry (K) to predict IOL power. It remains the most widely used formula globally because it is built into every biometer and familiar to every surgeon.
Best for: Normal eyes (AL 22–25 mm), especially when you have limited biometry data or are working in a setting where advanced formulas are unavailable.
Limitations: Progressively less accurate in very short eyes (< 22 mm) and long eyes (> 26 mm). Does not use anterior chamber depth (ACD), which is a significant predictor of effective lens position.
Hoffer Q — Short eyes
Published by Kenneth Hoffer in 1993, this formula was designed specifically to improve accuracy in short eyes and uses ACD in its calculation.
Best for: Axial length < 22 mm. Significantly outperforms SRK/T in this range.
Limitations: Less accurate in long eyes. Some studies show it over-corrects in eyes > 26 mm.
Holladay 1 — Normal to long eyes
The Holladay 1 formula improved on SRK/T by using a more sophisticated effective lens position (ELP) prediction based on both AL and K. It is well-validated in normal eyes and performs reliably in long eyes.
Best for: AL 22–26 mm, particularly good for long eyes in the 25–26.5 mm range where SRK/T begins to lose accuracy.
Haigis — Three constants, better ELP prediction
The Haigis formula uses three surgeon-specific constants (a0, a1, a2) and incorporates measured ACD directly into ELP prediction. It is the most sensitive formula to ACD variation.
Best for: Cases where ACD is unusual — flat anterior segments, deep anterior segments, or pseudoexfoliation where the lens-iris diaphragm position is unpredictable. Also reliable in long eyes.
Limitation: Requires optimization of all three constants against your own surgical outcomes — using published constants without optimization introduces systematic error.
Barrett Universal II — The modern standard
The Barrett Universal II (BUII) formula, developed by Graham Barrett, uses five biometric variables: AL, K, ACD, lens thickness (LT), and horizontal white-to-white (WTW) distance. It applies a theoretical model of the eye's optical system and predicts ELP using all available data.
Multiple large studies — including the EUREQUO registry analysis of over 600,000 eyes and the ESCRS biometry study — consistently show BUII has the lowest mean absolute error of any formula across all axial length ranges.
Best for: All eyes. BUII is currently the default recommendation of the ESCRS and the AAO for routine cataract surgery.
Limitation: Requires full biometry (LT and WTW in addition to AL, K, and ACD). Cannot be used if LT or WTW is unavailable.
Formula selection by axial length — a practical guide
| Axial length | First choice | Second choice | Avoid |
|---|---|---|---|
| < 21.0 mm (nanophthalmos) | Barrett Universal II | Hoffer Q | SRK/T, Holladay 1 |
| 21.0–22.0 mm (short) | Barrett Universal II | Hoffer Q | SRK/T |
| 22.0–24.5 mm (normal) | Barrett Universal II | Any | — |
| 24.5–26.0 mm (long-normal) | Barrett Universal II | Holladay 1 | — |
| > 26.0 mm (long) | Barrett Universal II | Haigis | Hoffer Q |
Special clinical situations
Post-refractive surgery eyes
Standard formulas are unreliable after LASIK, LASEK, or PRK because they rely on keratometry measurements that are altered by the refractive procedure. Use the Barrett True K formula (a variant of BUII), the Haigis-L formula, or the ASCRS online calculator that averages multiple post-refractive formulas.
Dense cataracts with unreliable biometry
Dense posterior subcapsular cataracts create signal noise in optical biometry. Use immersion ultrasound as a backup for AL measurement. Use the Holladay 1 or Haigis formula when optical biometry values are flagged as uncertain.
Irregular corneas
In keratoconus or corneal scarring, standard K measurements are unreliable. Use topography-derived mean K values and run multiple formulas — the agreement between formulas is a useful indicator of measurement reliability.
How Clinit handles IOL calculations
The Clinit optical module includes all five formulas on one screen. You enter AL, K, ACD, LT, and WTW from your biometer — or import them directly from IOLMaster and Lenstar via CSV. The module calculates IOL power for your target refraction across all five formulas simultaneously, so you can compare the results and identify outliers. Results are saved to the patient's surgical record with the biometry values used, the formula selected, and the surgeon's documented rationale. Pre-op and post-op refractions are linked to the IOL calculation for outcome tracking.


